
On April 6, 2026, the federal government released the 2027 Rate Announcement, or the Announcement of Calendar Year (CY) 2027 Medicare Advantage (MA) Capitation Rates and Part C and Part D Payment Policies. The Centers for Medicare & Medicaid Services (CMS) releases rate announcements as part of its annual rate-setting process for MA and Part D plans.
Medicare Advantage
2027 Payment Rate: A Welcome Improvement
Key Takeaways
- The 2027 Rate Announcement finalized a 5.33% effective growth rate with an expected average payment increase of 2.48%, (CMS’ 2.48% expected average change does not include the projected 2.50% increase in MA risk scores due to underlying coding trend), or over $13 billion in additional payments to MA plans
- This was an improvement over the proposed 4.97% effective growth rate with an expected average payment increase of only 0.09%
- Instead of the proposed flat payment, MA plans will have a payment increase from the federal government in 2027
The 2027 Advance Notice proposed a growth rate of 4.97% with a relatively flat payment average increase of only 0.09%, or about $700M in additional payments to MA plans. In the 2027 Rate Announcement, CMS finalized a 5.33% effective growth rate with an expected average payment increase of 2.48%, (CMS’ 2.48% expected average change does not include the projected 2.50% increase in MA risk scores due to underlying coding trend), or over $13 billion in additional payments to MA plans. This represents a 2.39 percentage-point improvement from the Advance Notice to the final Rate Announcement, which is above the average 1.02 percentage-point improvement measured from 2018–2026.
The larger increase could be attributed to several factors:
- CMS decided not to implement a new risk adjustment model for 2027, which eased risk score pressure by about 2%
- The finalized growth rate included additional data, including Original Medicare program experience and incurred dates through the fourth quarter of 2025
- CMS received a substantial 40,000+ comments* on the 2027 Advance Notice from stakeholders—including MA and Part D sponsors, advocacy groups, physicians, PBMs, pharmacies, and other interested parties, including LaborFirst’s own efforts to advocate for our clients
Medicare Advantage covers over half of eligible Medicare beneficiaries and continues to prove its staying power as an advantageous solution for group retiree plans. By increasing the average payment rate, CMS showed a forward-looking approach to Medicare Advantage. However, the base payment from Medicare is only one of several factors in an insurance carrier’s strategy for setting its premiums. Another factor is the utilization of healthcare services by its members. Utilization rates are increasing mostly due to a higher volume of physician and outpatient services, as well as prescription drugs.
Net Payment Impact
Year-to-Year Percentage Change in Payment Parameters
| 2027 Rate Announcement | 2026 Rate Announcement | 2025 Rate Announcement | |
| Effective Growth Rate | 5.33% | 9.04% | 2.33% |
| Rebasing/Re-pricing | -0.17% | -0.28% | 0.07% |
| Change in Star Ratings[1] | -0.03% | -0.69% | -0.11% |
| MA Coding Pattern Adjustment | 0% | 0% | 0% |
| Risk Model Revision & FFS Normalization[2] | -1.12% | -3.01% | -2.45% |
| Expected Average Change[3] | 2.48% | 5.06% | 3.70% |
[1] Change in Star Ratings reflects the estimated effect of changes in the Quality Bonus Payments for the upcoming payment year.
[2] The impact of the update to the Fee-for-Service (FFS) normalization factors for MA risk adjustment is not shown above separately because there is considerable interaction between the impact of the MA risk adjustment model updates and the normalization factor update. Therefore, the combined impact is shown above.
[3] The overall expected average change does not include an adjustment for underlying coding trend in MA. For CY 2027, CMS expects the MA risk scores to increase, on average, by 2.50% due to the underlying coding trend.
*Announcement of Calendar Year (CY) 2027 Medicare Advantage (MA) Capitation Rates and Part C and Part D Payment Policies. cms.gov, 6 April 2026, https://www.cms.gov/files/document/2027-announcement.pdf
Part C Risk Adjustment Model: A Step Toward Stability
Key Takeaways
- CMS will keep the current CMS-HCC model (V28)
- To curb insurers from “upcoding,” unlinked chart reviews and audio-only encounters will be excluded from risk score calculation with one exception for members who switch from one MA organization to another
- Without the exception, the impact of excluding unlinked diagnoses would be -1.78%
- The impact of excluding audio-only services would be 0%, on average
The 2027 Advance Notice proposed several changes to the current Part C risk adjustment model (2024 CMS-HCC). The most impactful change would have been updating the timeframe of the underlying data to reflect current costs. CMS proposed updating the underlying Original Medicare data to use diagnoses from 2023 FFS claims, predicting 2024 expenditures (from 2018 and 2019, respectively, which are pre-pandemic datasets). CMS also proposed to update the denominator year to 2024 (from 2020). The use of more recent data would have resulted in three points of additional risk score pressure and about a 2% reduction in payments to MA plans.
In a positive move toward program stability, CMS did not finalize this change in the 2027 Rate Announcement. Keeping the same risk model significantly improved the financial outlook for MA plans. The three projected points of risk score pressure is now finalized at just over one point. Carriers and providers also have more time to adapt to the current CMS-HCC Model Version 28 (V28), phased in between 2024 and 2026.
Another proposed change in the 2027 Advance Notice was the exclusion of diagnosis information from audio-only encounters and “unlinked” chart review records, or those not associated with a specific encounter. Plans can continue to submit unlinked chart reviews, but those diagnoses alone would no longer count toward risk score calculation. Insurers would use a qualifying provider encounter to prove delivery of corresponding care. CMS intended goal is to curb insurers from “upcoding” enrollees in order to increase their payout.
The proposed exclusion of diagnosis information from audio-only encounters and “unlinked” chart review records was finalized with one exception for members who switch from one MA organization to another. This exception is important to carriers for preserving continuity in risk scores for transitioning members and reducing potential disruption for MA plans experiencing churn. Without the exception, it would have been more difficult for members to transition from their current carrier because there would have been a lack of data, resulting in increased costs. The impact of excluding unlinked diagnoses from risk scores is projected to be -1.78% without the exception, and the impact of excluding audio-only services is projected to be 0%, on average.
Medicare Part D
Defined Standard Benefit: Increased Thresholds Are Still Low in Comparison
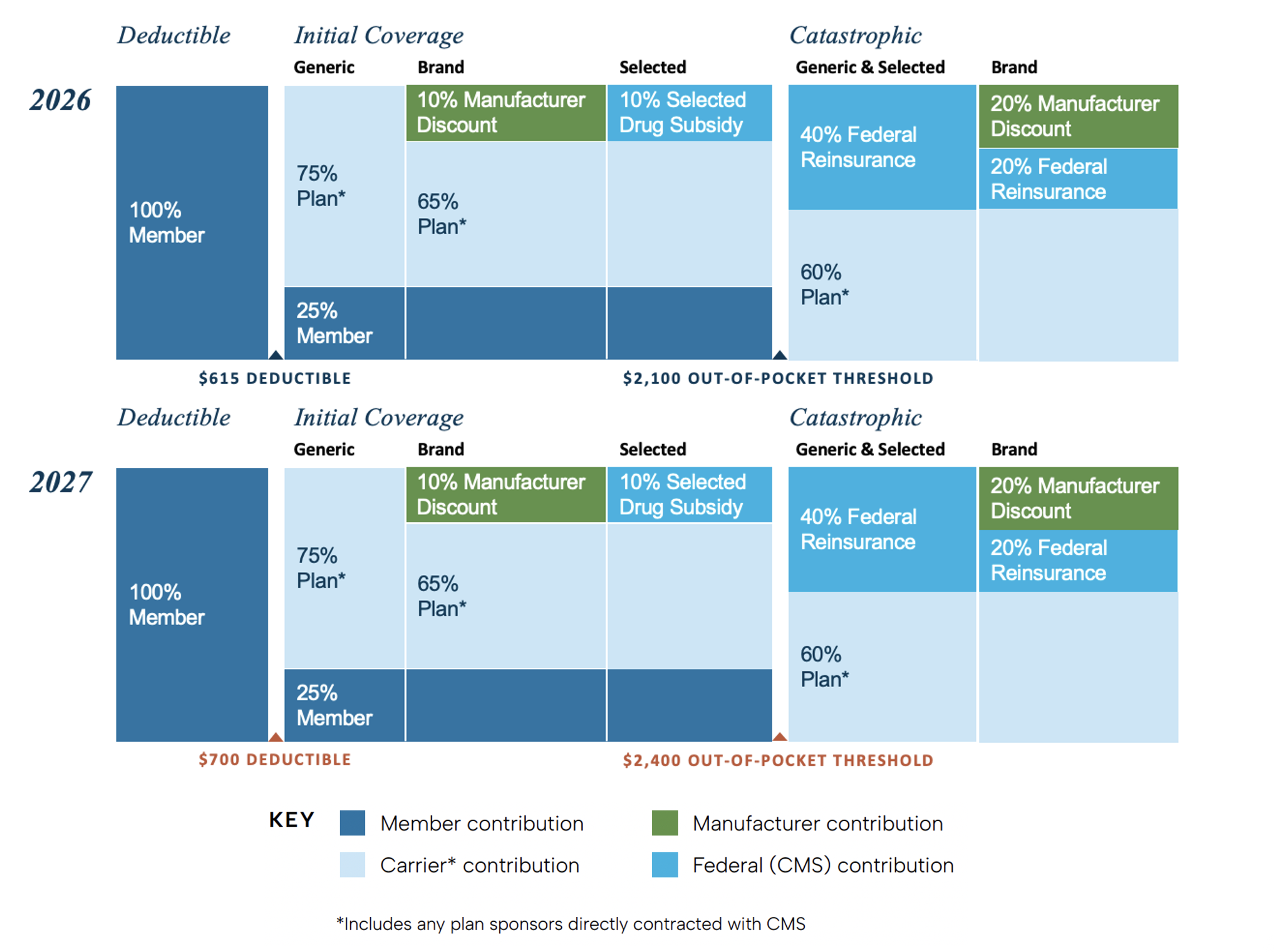
The Medicare Part D standard benefit is defined by the financial structure of its cost-sharing. In 2027, CMS will increase the standard deductible for Part D enrollees to $700 (up from $615) and the standard out-of-pocket (OOP) spending cap to $2,400 (from $2,100). The 2027 OOP threshold remains far below the pre-IRA catastrophic threshold, which was roughly $8,000 in TrOOP. However, TrOOP included amounts beyond direct member cost-sharing, such as applicable manufacturer discounts. There are no other changes to the structure or funding contributions for 2027.
Changes to Part D
Part D Risk Adjustment Model: Updates to More Recent Data
Key Takeaways
- CMS did finalize the update to use more recent underlying data in the Part D risk adjustment model
- To curb insurers from “upcoding,” unlinked chart reviews and audio-only encounters will be excluded from risk score calculation
- CMS will continue to use different normalization factors for standalone PDP and the Part D in an MAPD plan
As with the Part C risk adjustment model, CMS is also excluding diagnoses from audio-only services and unlinked chart review records from risk score calculation. For most organizations, with the exception of PACE organizations (Program of All-Inclusive Care for the Elderly), there will be an exception for members who switch from one MA organization to another.
Unlike the Part C risk adjustment model, CMS did finalize the update to the timeframe of the underlying data in the Part D risk adjustment model (CMS-RxHCC). The underlying Original Medicare data will use diagnoses from 2023 FFS claims and MA encounter data records and gross drug costs from 2024 Prescription Drug Events, or PDEs (from 2022 diagnoses and 2023 costs). CMS will also update the denominator year to 2024 (from 2023). With these changes, the Part D risk adjustment model will be different from the Part C risk adjustment model.
In 2027, CMS will continue to use different normalization factors for PDP vs MAPD plans. Some carriers and consultants have explored unbundled MA-only plus PDP structures for larger groups where separate PDP treatment may produce more favorable economics. For the 2027 plan year, unbundling an MAPD plan may produce more favorable economics. CMS continues to evaluate MAPD and PDP risk adjustment differences, including separate normalization factors.
For an overview of policy and technical changes to Group Medicare Advantage and Part D in 2027, watch a recording of our webinar “Understanding Medicare’s 2027 Final Notice & Final Rule.” In addition to the 2027 Rate Announcement, we cover Star Ratings, Medicare GLP-1 Bridge and BALANCE Model programs, Retiree Drug Subsidy, and more.
The CY 2027 MA and Part D Rate Announcement may be viewed at:
https://www.cms.gov/files/document/2027-announcement.pdf
Connect with us to learn more:




